Discharge Intel
Clinical Intelligence for Health Plans
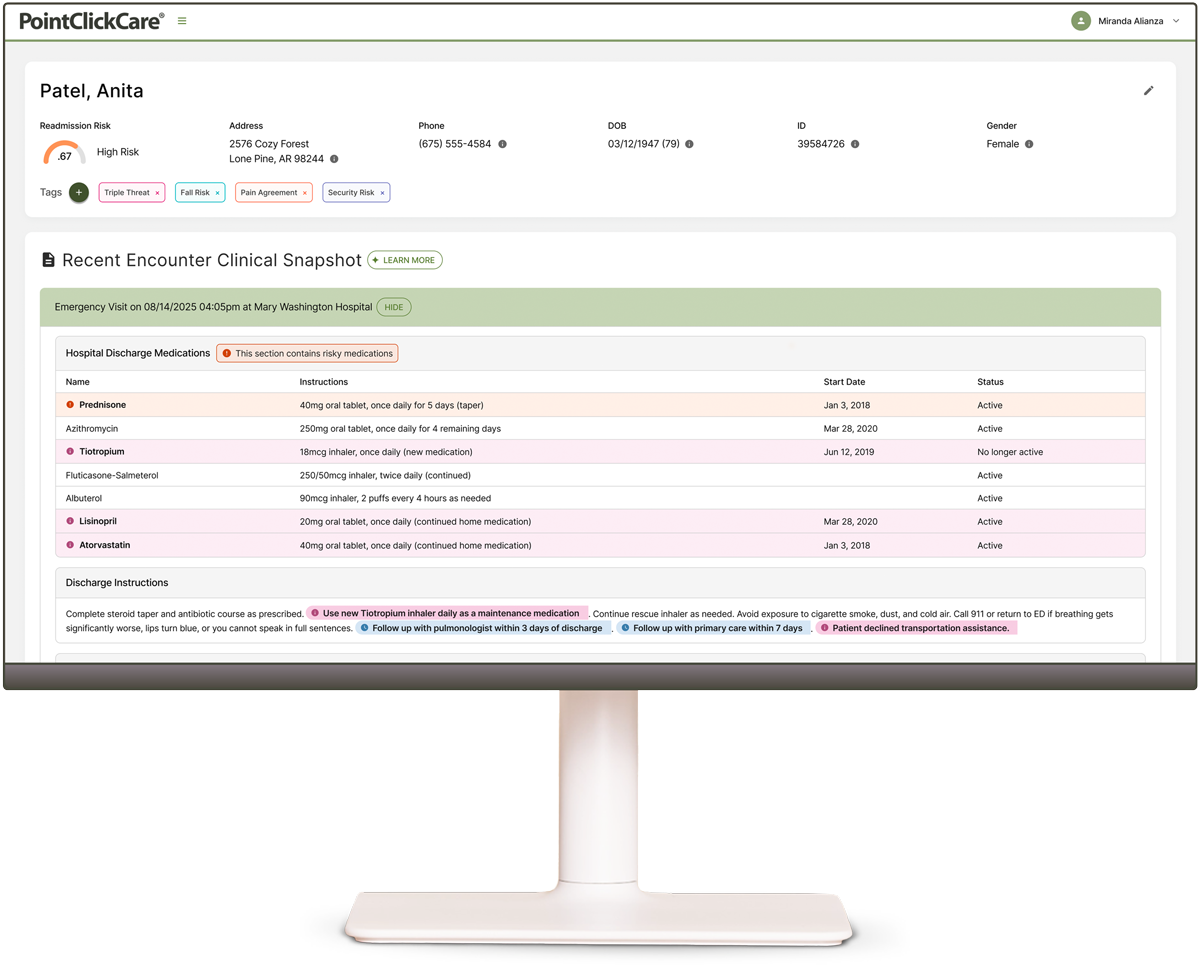
When data arrives too late, it’s no longer intelligence. The first 48 hours after discharge shape cost and quality outcomes. Discharge Intel uses AI to surface actionable clinical insights within 24 hours of inpatient or ED discharge, so care teams can act while there’s still time to influence outcomes.
Clinical Intelligence When It Matters Most
AI That Does the
Work
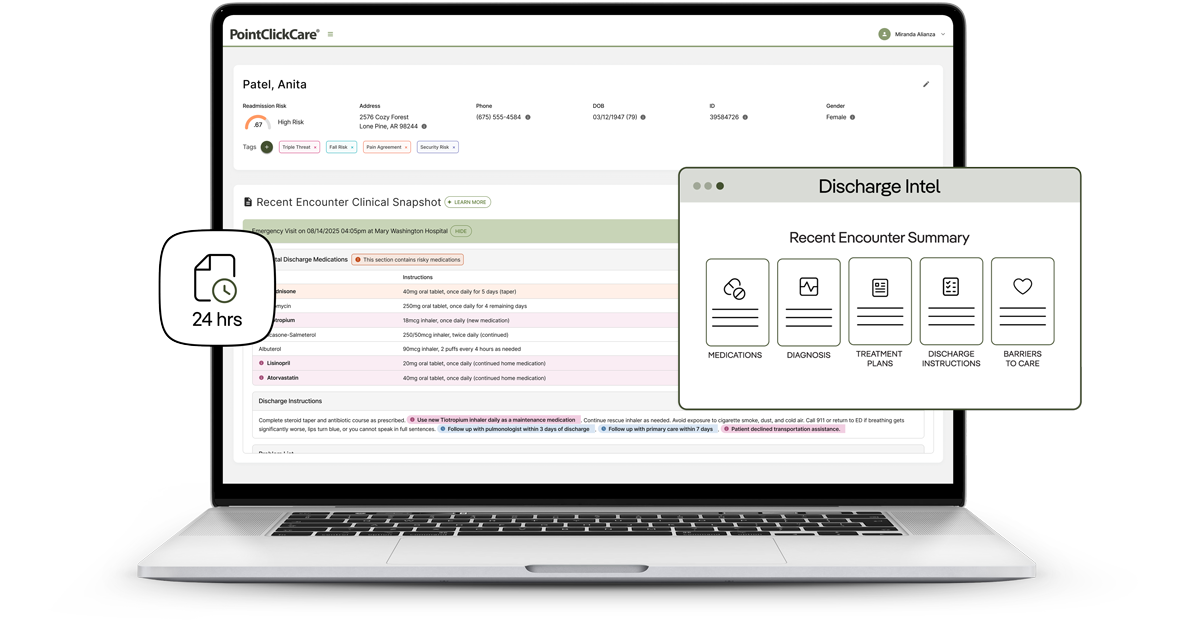
Distills complex and unstructured clinical documentation to surface key meds, follow-ups, instructions. No more digging.
Intelligence in 24 Hours
Clinical context within 24 hours reaches your team when intervention has the greatest impact on outcomes. Data that arrives late is just history.
Coverage Across any EHR
Your members don’t stay in one system—your visibility shouldn’t either. 2,800+ hospitals, 3,600+ clinics. One unified, EHR-agnostic view.
Built for Care Managers
Ready to power workflows from day one. Clinical intelligence organized around what care managers need to act, ready when they pick up the phone.
Transform Care Management From Reactive to Ready
Readmissions Prevented. Costs Controlled.
Catch medication risks before they readmit
Medication issues are a leading driver of preventable readmissions. Without knowing what changed at discharge—a new prescription, a discontinued medication, a dangerous interaction—care managers can’t intervene before problems escalate. At $17,500+ per readmission, timely clinical context enables intervention that prevents costly events.
Act inside the immediate post-discharge window
Clinically informed intervention during the immediate post-discharge window reduces ED bounce-backs, prevents unnecessary utilization, and lowers total cost of care.
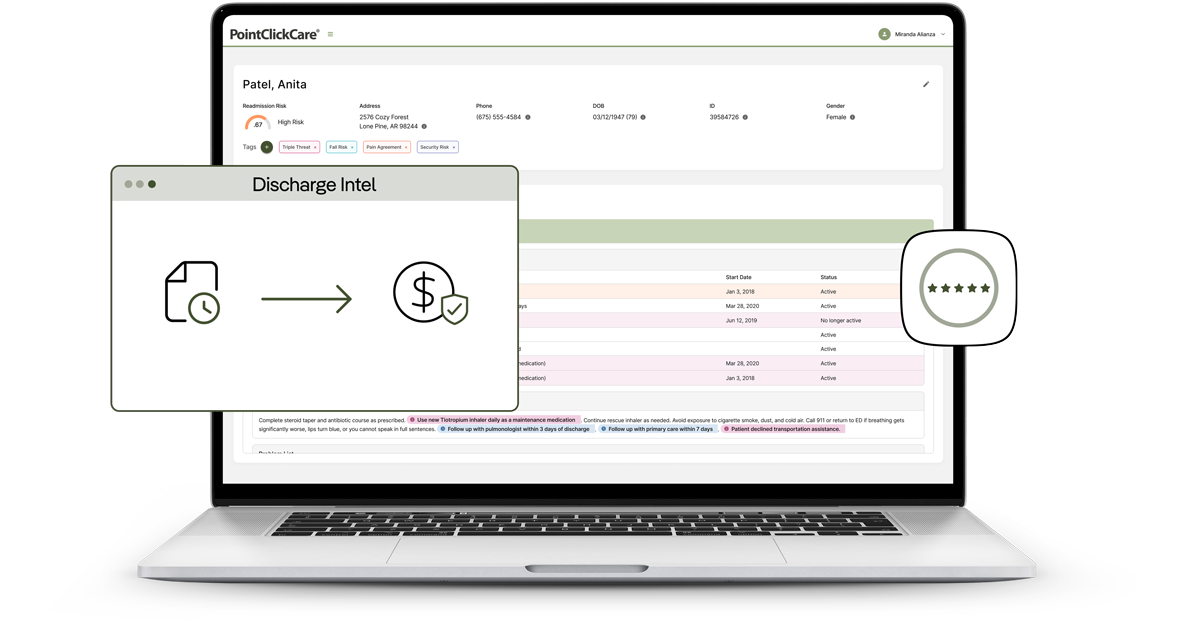
Quality-Linked Revenue Protected
Start outreach with clinical context
Time-critical HEDIS measures (TRC, FUM, FUH, FUA, and more) operate within narrow windows. When the first outreach call is spent gathering basic information instead of addressing barriers, care gaps stay open past the measurement deadline, and quality-linked revenue is lost. Clinical context within 24 hours of hospital discharge enables care managers to close gaps while measurement windows are still open.
Star ratings depend on what happens after discharge
With measures like Plan All Cause Readmissions triple-weighted in CMS Star ratings, plans need every tool at their disposal to prevent readmissions. Equiping care managers with clinical context at the point of invervention is what is missing to protect quality-linked revenue.
Trust That Drives Follow Through.
From information gatherer to trusted advisor
75% of health plans say care managers are seen as information gatherers, not trusted advisors. When managers call already informed—especially for vulnerable members—conversations feel guided, not interrogative, helping build trust and follow‑through.
Lift CAHPS through informed outreach
CAHPS scores reflect how members experience their health plan. When post-discharge outreach starts with clinical context instead of questions, members feel supported, not surveyed. Informed care managers drive the positive interactions that lift CAHPS performance.

Readmissions Prevented. Costs Controlled.
Catch medication risks before they readmit
Medication issues are a leading driver of preventable readmissions. Without knowing what changed at discharge—a new prescription, a discontinued medication, a dangerous interaction—care managers can’t intervene before problems escalate. At $17,500+ per readmission, timely clinical context enables intervention that prevents costly events.
Act inside the immediate post-discharge window
Clinically informed intervention during the immediate post-discharge window reduces ED bounce-backs, prevents unnecessary utilization, and lowers total cost of care.
Quality-Linked Revenue Protected
Start outreach with clinical context
Time-critical HEDIS measures (TRC, FUM, FUH, FUA, and more) operate within narrow windows. When the first outreach call is spent gathering basic information instead of addressing barriers, care gaps stay open past the measurement deadline, and quality-linked revenue is lost. Clinical context within 24 hours of hospital discharge enables care managers to close gaps while measurement windows are still open.
Star ratings depend on what happens after discharge
With measures like Plan All Cause Readmissions triple-weighted in CMS Star ratings, plans need every tool at their disposal to prevent readmissions. Equiping care managers with clinical context at the point of invervention is what is missing to protect quality-linked revenue.
Trust That Drives Follow Through.
From information gatherer to trusted advisor
75% of health plans say care managers are seen as information gatherers, not trusted advisors. When managers call already informed—especially for vulnerable members—conversations feel guided, not interrogative, helping build trust and follow‑through.
Lift CAHPS through informed outreach
CAHPS scores reflect how members experience their health plan. When post-discharge outreach starts with clinical context instead of questions, members feel supported, not surveyed. Informed care managers drive the positive interactions that lift CAHPS performance.
Before Discharge Intel, we had no visibility and were flying blind. Our team spent 20 minutes per case calling hospitals, faxing requests, and waiting days for discharge summaries. Now we get the information the same day, act proactively, and have better, more informed conversations with members, which has helped drive about a 60% engagement rate.
Director of Case Management
Regional Medicare Advantage Health Plan
20+
Minutes saved per case
60%
Engagement rate

Request a Demo
Book a live demonstration to see how Discharge Intel can help your organization transform care management with clinical intelligence delivered within 24 hours of discharge.
Additional Solutions for Discharge Intel
See All Relevant SolutionsFrequently Asked Questions
Discharge Intel delivers actionable clinical intelligence within 24 hours of an emergency department or inpatient hospital discharge. This includes AI-powered clinical snapshots summarizing medications, discharge instructions, follow-up requirements, and more—reaching your care team during the critical post-discharge window when intervention has the greatest impact on outcomes.
Discharge Intel uses AI to distill pages of clinical discharge documentation into an actionable summary. This includes key medications and changes, discharge instructions, treatment plans, diagnoses, follow-up requirements, and problem lists. Full clinical documentation—including the complete encounter-level continuity of care document (CCD)—is always accessible for deeper review. The goal: care managers pick up the phone already knowing the clinical story, so the conversation starts with guidance, not questions.
Yes. Discharge Intel is powered by PointClickCare’s EHR-agnostic network spanning 2,800+ hospitals, 3,600+ clinics, and over 100 million member lives. It delivers clinical intelligence regardless of where your members receive care. Your members don’t stay in one system—your clinical visibility shouldn’t either.
Time-critical HEDIS measures require action within narrow windows after discharge. Discharge Intel delivers the clinical context care teams need—medications, follow-up requirements, and barriers to care—while those windows are still open. Faster access to clinical documentation enables care managers to close gaps within measurement windows, supporting stronger HEDIS performance, improved Star Ratings, and the quality-linked revenue tied to them.


Take a Closer Look
Request a demo of Discharge Intel and see the difference AI-powered clinical intelligence can make for your organization.
See Discharge Intel in Action
Watch a short on-demand demo to preview how Discharge Intel helps health plans reduce readmissions, lower costs, and strengthen HEDIS performance.