
California’s D-SNP Expansion Changed the Stakes for Medi-Cal Plans. Here’s How to Get Ahead.
 11 min
11 min
For many California Medi-Cal managed care plans, 2026 brought a new level of accountability: Medicare performance is now part of their operating reality.
Under CalAIM’s EAE model, California Medi-Cal managed care plans are now required to operate, or be affiliated with, a D-SNP. That requirement brings Medicare and Medi-Cal under the same organizational umbrella for dual-eligible members. That shift became much more immediate in January 2026, when California expanded D-SNP from 12 counties to 41. For many plans, that has meant stepping into Medicare Stars accountability sooner and at a broader scale than they anticipated.
This post is for plans that have spent years, maybe decades, managing their Medi-Cal population well and are now being asked to navigate a new and unfamiliar set of rules. What we see consistently is this: the population may be familiar, but managing it under Medicare quality accountability is a different operational challenge.
You’ve Managed This Population. You Haven’t Managed Them Under Medicare.
There’s an important distinction to make upfront: the dual-eligible population is not new to you. You know these members. You’ve coordinated their long-term supports, behavioral health, and community-based services. You’ve built care models around their complexity.
What is new is who’s measuring performance and what is now riding on it.
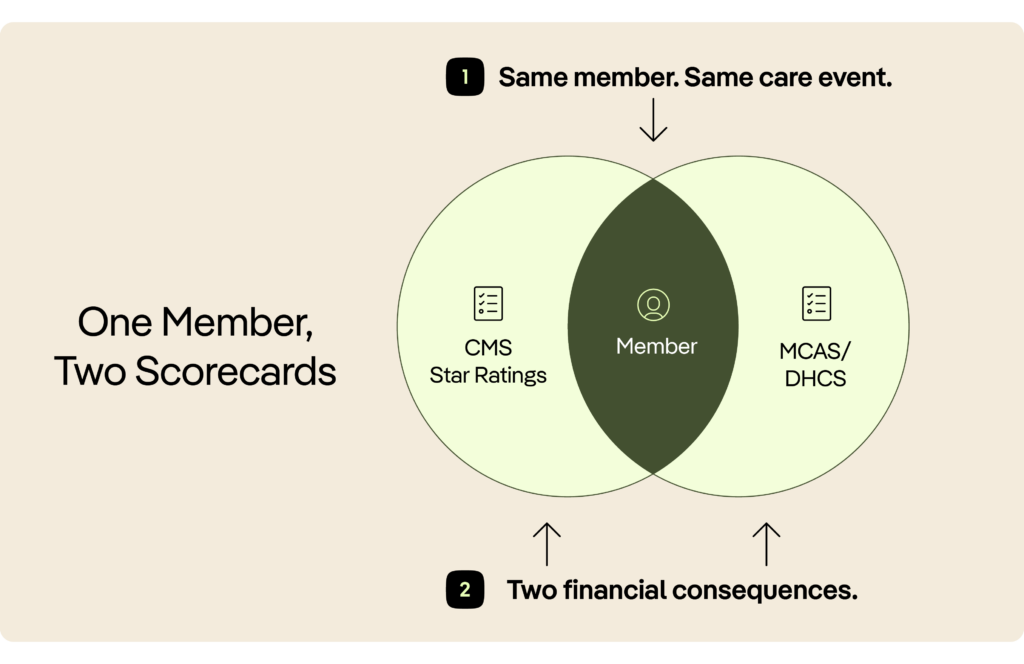
Under EAE, you’re now simultaneously accountable to two independent quality systems:
- CMS Star Ratings, which govern your Medicare D-SNP contract
- MCAS (Medi-Cal Managed Care Accountability Set), which governs your DHCS contract
Both systems measure many of the same members, and both carry real financial consequences. That overlap is where the pressure builds. A single failed care transition, such as a missed follow-up, a delayed notification, or a member lost in post-acute care, can affect both scorecards at once.
That is the new math: one member, two P&Ls, and simultaneous accountability.
What Makes Dual Eligibles So Operationally Complex
That pressure is especially acute with dual-eligible members. They represent roughly 15–20% of Medicare enrollment nationally, but they account for a disproportionate share of total cost. In California, they are among the highest-cost, highest-complexity populations in the health system. Now they are your responsibility under a framework most California MCPs have never had to operate in before.
Here’s what makes them uniquely challenging to manage under Medicare quality standards:
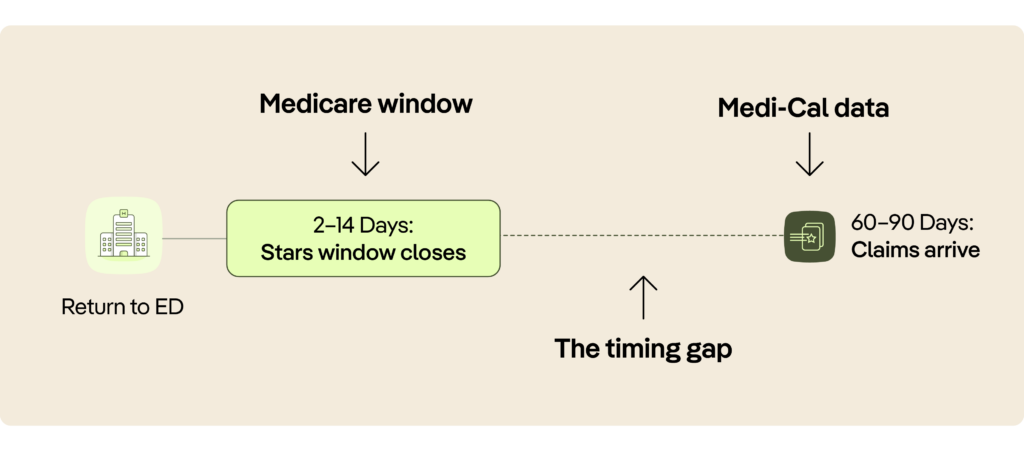
They move through care settings constantly. They move from hospital to SNF, from SNF to home, and from home back to the ED. Each of these transitions creates a moment when quality measures open or close. If you are not watching in real time, they can quietly fail.
They have long post-acute stays. D-SNP members have higher SNF utilization and longer lengths of stay than typical Medicare Advantage populations. That means more time in a care setting where, historically, health plans have had almost no visibility.
They are heavy ED users. They often visit the ED for conditions that could be managed in community settings. Every avoidable ED visit is both a quality event and a cost event. Under EAE, it affects your Medicare and Medi-Cal P&L at the same time.
Their data arrives late. Claims-based workflows, the backbone of most Medi-Cal care management operations, often run 60 to 90 days behind. In Medicare Stars, compliance windows are measured in days. That gap is where performance slips away.
The Measures That Matter Most Right Now
That complexity quickly shows up in the measures that matter most. You do not need to master the entire Stars framework on day one. But there are a handful of measures with outsized revenue impact that every new D-SNP plan should understand immediately.
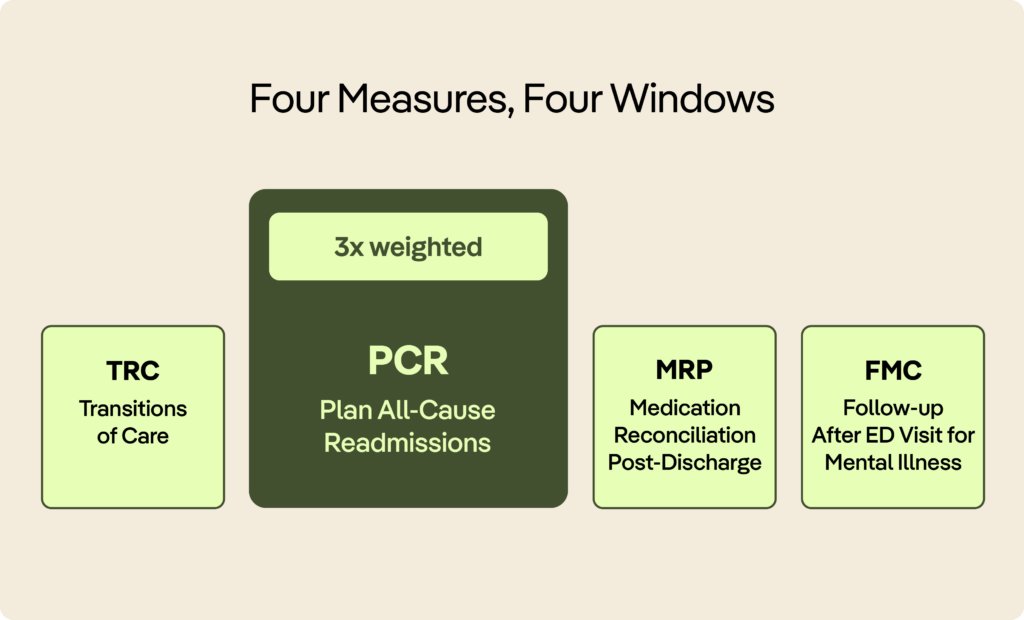
Transitions of Care (TRC) is the foundational post-discharge measure. It requires that the attributed primary care provider receives notification of an inpatient admission and discharge documentation within two calendar days. Every hospital stay involving a D-SNP member creates a time-sensitive obligation for your plan. At scale, across thousands of members, this is not something you can manage manually through faxes and phone calls.
Plan All-Cause Readmissions (PCR) is now triple-weighted in the Stars calculation, the highest multiplier of any single measure. Every avoidable readmission does more than lower your PCR score. It creates real cost, real risk, and real revenue loss.
Medication Reconciliation Post-Discharge (MRP) is one of the most underperforming measures across plans nationally and one of the most actionable. Your pharmacy team needs timely visibility into medication changes within a narrow post-discharge window. Most teams do not get that information until claims arrive.
Follow-up After ED Visit for Mental Illness (FMC) is especially relevant for dual-eligible populations, which have significantly higher rates of behavioral health diagnoses. This measure is often missed because ED visits are not always visible to the plan in time.
The Visibility Gap Is the Real Problem
Once plans understand the measures, the next challenge becomes clear: they cannot see enough, soon enough, to manage them well.
They do not know when a member is discharged from the hospital. They do not know what medications changed, what follow-up was ordered, or what the discharging team observed clinically. When a member moves to a skilled nursing facility, visibility often drops to zero. Care managers call facilities, wait for faxed documentation, and piece together a clinical picture from fragments, often days after the window to intervene has already closed.
The result is care management that is largely reactive. By the time your team knows a quality event has occurred, the measure window may already be closed, the readmission may already have happened, or the member may already have returned to the ED.
You cannot manage what you cannot see. And for most California plans entering D-SNP for the first time, the infrastructure to see this population in real time simply doesn’t exist yet.
That is not a criticism. It is an honest description of where much of the market is today. The real question is how quickly you can change it.
What “Good” Looks Like for a New D-SNP Plan
That is why the strongest plans focus less on heroic manual effort and more on building the right operating model from the start. In their first year of Medicare Stars accountability, they tend to share a few characteristics that set them apart.
They know about discharges in real time. They know this not from claims or weekly reports, but from live alerts that tell the right care team, at the right moment, that a member has been discharged from a hospital or ED and needs action.
Their care managers have clinical context before they pick up the phone. The outreach call is not just an information-gathering exercise. It is an intervention. Medication changes, diagnoses, follow-up orders, and flagged high-risk medications are already in front of the care manager before they dial.
They can see their members during the post-acute stay. They know where their members are in skilled nursing. They know how they are progressing. They get early warning when a member is at risk of returning to the hospital, which gives them time to work with the facility and prevent it.
Provider notification is automated, not manual. TRC requires that the PCP receive admission notification and discharge documentation within 48 hours. At any meaningful scale, that standard cannot be met through manual coordination alone. Plans that do this well have automated the workflow.
They can prioritize. When a population triples in size overnight, care managers cannot reach everyone. Plans that succeed have a reliable way to surface the highest-priority members, including those in an open measure window, those with the most time-sensitive gaps, and those at highest risk of readmission. That is how they direct resources where they matter most.
This Is Not a D-SNP-Only Investment
That operating model does more than support D-SNP. One of the most important things to understand about the infrastructure you’re building now is that it does not stay confined to this one line of business.
The capabilities that let you manage D-SNP members well, including real-time discharge notification, clinical summaries from inpatient and ED encounters, post-acute visibility, and care gap prioritization, are the same capabilities you need across your entire Medicare Advantage book and your broader Medi-Cal population.
D-SNP may be the reason the investment gets approved and the infrastructure gets built. But the return extends across every line of business where care transitions shape quality and cost outcomes.
For plans that have operated primarily in Medi-Cal, this may be the first time you’ve had real-time visibility into the acute and post-acute episodes your members experience. That visibility doesn’t just help you hit Stars targets. It fundamentally changes how you manage your population.
The Window to Get This Right Is Narrow
That broader value matters because the timeline is already tight. California’s D-SNP expansion happened in January 2026, and CMS measurement is already underway. The quality record your plan builds this year, including the baselines you set, the measures you close, and the readmissions you prevent or fail to prevent, will shape your competitive position for years.
Plans with 4+ Star ratings receive a 5% benchmark increase from CMS. At the enrollment scale of a large California county plan, that quality bonus is worth millions of dollars annually. More importantly, it compounds: higher ratings drive higher enrollment, which drives more revenue, which funds better care. The inverse is also true.
Twenty-two of 25 California Medi-Cal managed care plans received MCAS sanctions in one recent measurement year. Plans that build Medicare quality infrastructure now, before the measurement window closes, will be in a fundamentally different position from those that wait.
The good news is that the gap between where most California D-SNP plans are today and where they need to be is not insurmountable. The operational model exists. The technology exists. The path is clear.
What it requires is moving quickly, with the right infrastructure, before Year 1 becomes a baseline you spend years recovering from.

Get Earlier Visibility Into the Transitions That Drive Performance
PointClickCare helps health plans act on the moments that matter most, with real-time clinical data across a network of 2,800+ hospitals, 27,000+ long-term and post-acute care facilities, and 3,600+ ambulatory clinics. That visibility helps plans move faster on transitions of care, close time-sensitive quality gaps, and manage the post-acute episodes that drive readmissions and total cost.
If you’re building Medicare quality infrastructure for the first time, it helps to see where timely action can create the greatest lift. We’d welcome the chance to show you how real-time signals, clinical context, and prioritized workflows can help your team respond sooner and perform with more confidence.
Read to see what that could look like in practice?
Share a few details below to get a personalized view of how PointClickCare can help your team act earlier, focus resources where they matter most, and strengthen performance across the transitions that shape quality outcomes.
Our Author

Kai-Yun Kao is Market Director at PointClickCare, where she serves as a strategic leader responsible for driving integrated market growth across the full PCC portfolio in her territory. With over a decade of experience in health IT and Medicaid policy, she has built her career at the intersection of state policy, health information exchange, and care coordination.
At PointClickCare — including her time at Audacious Inquiry prior to its 2022 acquisition — Kai-Yun has led cross-functional teams to expand acute data coverage, grow market revenues, and bring new products to market. Earlier in her career, she served as Lead Policy Analyst for the Maryland Medicaid EHR Incentive Program, overseeing health IT policy implementation and managing large-scale state health information systems. She holds a Master of Arts in Public Policy from Johns Hopkins University.




